Scrub Typhus is an acute febrile illness which is caused by an obligate intracellular pathogen called Orientia tsutsugamushi, which is transmitted by the bite of infected larval stage trombiculid mite, Leptotrombidium spp. (Chiggers). The name scrub typhus was applied after discovery of increased frequency of the disease in scrub or wasteland areas.
Etiology of Scrub Typhus
Orientia tsutsugamushi is the causative agent of Scrub Typhus. It has following characteristics:
- They are obligate intracellular pathogens which needs to infect eukaryotic cells in order to multiply.
- Initially, they were categorized under genus Rickettsia, but now classed in a separate genus known as Orientia.
- They are 0.5 to 0.8 µm wide and 1.2 to 3.0 µm long.

- They are rod shaped bacterium.
- They can be cultured in cell monolayers.
- Gram Staining is not preferred but if done may appear as gram negative bacteria.
- Gimenez stain is preferred.
- The organism is highly virulent and should only be handled in a laboratory with biosafety level 3 facilities.
- They exhibit extensive genomic and antigenic heterogeneity that may lead to the definition of multiple species in the genus.
- Their genome is approximately 2000 kb.
- They are found throughout the mites body but is present in the greatest number in salivary glands.
- There are numerous serotypes, among which 5—Karp, Gilliam, Kawazaki, Boryon, and Kato—are helpful in serologic diagnosis.
- This pathogen does not have a vacuolar membrane; thus, it grows freely in the cytoplasm of infected cells.

Epidemiology of Scrub Typhus
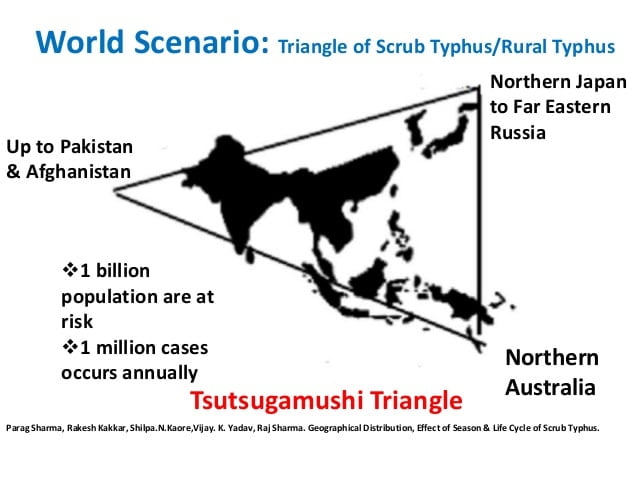
- They are endemic across extensive part of Asia, South Asia, Australia and the Pacific.
- It is found in India, Pakistan, China, Thailand, Malaysia, Taiwan, Tibet, Japan, Russia, South Korea and Nepal.
- These regions in which scrub typhus is endemic is referred as the tsutsugamushi triangle.
- They were clinically described in the Far East more than 1500 years ago.
- Over 1 Billion people are living in endemic areas and as many as 1 million are infected annually.
- Scrub typhus was first described in China in 313 AD and first isolated in Japan in 1930. Before 1986, Scrub Typhus was only found in southern china primarily in summer. In 1986, it was first reported in Mengyin County, Shandong Province, China.
- During World War II, 18,000 cases were observed in Allied troops stationed in rural or jungle areas of the Pacific theatre.
- In Nepal, there were 400 cases and at least 5 people have died till the data of 20th Sept, 2016.
Sign and Symptoms of Scrub Typhus
The incubation period can be from 6 to 20 days (Average 10 days).

Symptoms includes:
- Papule followed by an eschar at the site of chigger feeding (only in 50%)
- Fever
- Headache
- Myalgia
- Cough and Lung infection
- Diarrhea, abdominal pain, nausea and vomiting
- Regional lymphadenopathy
- Maculopapular rash
- Blood-shot eyes
- Indigenous patients do not commonly develop rash or lymphadenopathy which is thought to be related to previous exposure
- Severe cases can develop encephalitis and interstitial pneumonia and this may be fatal. If concomitant G6PD deficiency is present then the severity is increased.
Pathogenesis of Scrub Typhus
- Mortality rate ranges from 6.1% to 25% in Southeast Asia.
- Scrub typhus fever is not spread from person-to-person.
- Scrub typhus is spread from one person to another by the bite of a mite (called a “chigger”) infected with Orientia tsutsugamushi.
- The larva (chigger) is the only stage that can transmit the disease to humans and other vertebrates, since the other life stages (nymph and adult) do not feed on vertebrate animals.
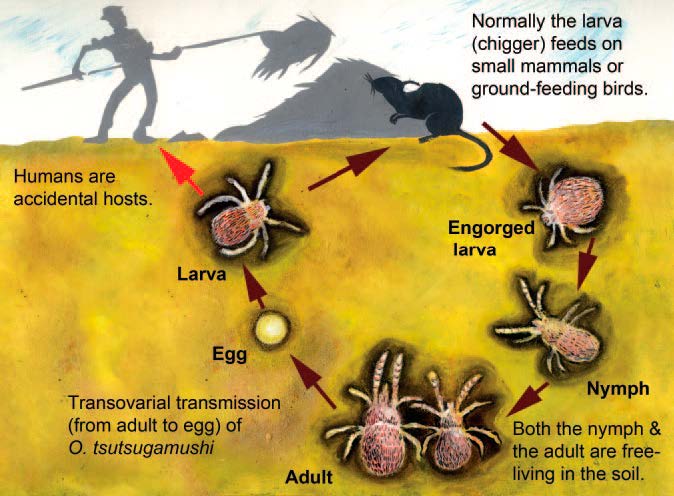
Figure: Life cycle of a Leptotrombidium mite
- These mites passes the infection to humans by feeding on the fluid in skin cells.
- Endothelial cells of most organs including skin, heart, lung, brain, kidney, pancreas, have been presented as the target cells of O. tsutsugamushi.
- They have been located within cardiac muscle cells and in macrophages of liver and spleen.
- The bacteria multiply at the inoculation site, and a papule forms that ulcerates and becomes necrotic, evolving into an eschar, with regional lymphadenopathy that may progress to generalized lymphadenopathy within a few days.
- O. tsutsugamushi stimulates phagocytosis by the immune cells, and then escapes the phagosome.
- It replicates in the cytoplasm and then buds from the cell.
- The bacteria are able to harness the microtubule assembly inside the human cell for movement.
- Antibody-opsonized bacteria are still able to escape the phagosome but cannot effectively move on the microtubule; as a result, overall infectivity is decreased.
- Scrub typhus may disseminate into multiple organs through endothelial cells and macrophages, resulting in the development of fatal complications.
- One study conducted in adult Thai patients have suggested that Orientia tsutsugamushi induces a type 1 immune response, associated with elevation of interferonalpha, IL-18 and IL-15 levels.
- During the initial inflammatory response to infections, early response cytokines (tumour necrosis factor-alpha, interleukin (IL)-1beta and IL-6) up-regulate cellular adhesion molecules (CAMs) on the surface of host leucocytes and endothelial cells (EC), which co-ordinate leucocyte transmigration across the endothelium.
- The selectins mediate initial leucocyte contact with EC, capturing cells from the bloodstream, followed by characteristic rolling and firm tethering to the endothelium. This requires higher-affinity leucocyte integrins (LFA-1 and Mac-1) binding to members of the immunoglobulin (Ig) superfamily, intercellular adhesion molecule-1 (ICAM-1) and vascular adhesion molecule-1 (VCAM-1), which are expressed on activated EC, enabling subsequent leucocyte diapedesis.
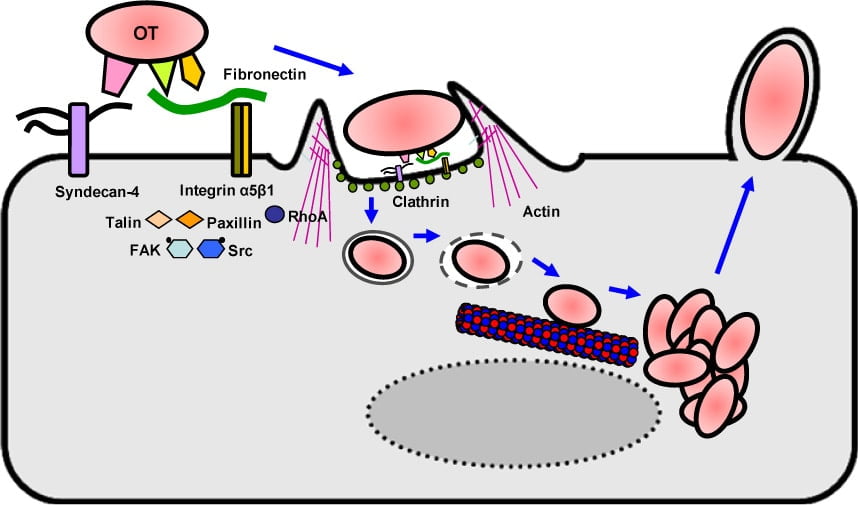
Figure: Hypothetical model for the intracellular invasion of O. tsutsugamushi
Diagnosis of Scrub Typhus
Specimens: Skin or lymph node biopsy, Heparinized blood, EDTA blood, Serum
- Immunofluorescence and immunoperoxydase assays
- Rapid immunochromatographic Flow Assay (RFA)
- Dot blot immunoassay
- The Weil-Felix test using the cross reactivity of O. tsutsugamushi with Proteus OX-K is still used in endemic areas despite its poor sensitivity and specificity.
- Orientia tsutsugamushi can be cultivated on L929 cells.
- ELISA
- PCR (Polymerase Chain Reaction)
- Sequencing of the 56-kDa protein gene
Treatment of Scrub Typhus
- The tetracyclines and chloramphenicol remain the standard treatment for scrub typhus.
- Doxycycline is used orally (100 mg twice daily for 7 days) or chloramphenicol in more severe cases (500 mg every 6 hours for 7 days or 50-75/mg/kg/day in children).
- Azithromycin has been used in resistant cases and may be better than doxycycline – especially in children and pregnant women.
- There are no vaccines available for Orientia tsutsugamushi.
Prevention and Control of Scrub Typhus
- Avoiding the bites of chiggers
- Wearing long sleeves,
- Not sitting directly on the grass,
- Keeping your clothes off the grass,
- Using insect repellents applied to the skin and clothing containing dibutyl phthalate, benzyl benzoate, diethyl toluamide.
- A weekly dose of 200 mg doxycycline is also effective in the prevention of scrub typhus.
- Clearing the vegetation where rats and mice live
- Health education of the people regarding the modes of transmission and personal prophylaxis is of paramount importance and can go a long way in prevention of the disease.
References
- https://emedicine.medscape.com/article/971797-overview#a5
- https://en.wikipedia.org/wiki/Scrub_typhus
- https://www.healthline.com/health/typhus
- https://www.merckmanuals.com/professional/infectious-diseases/rickettsiae-and-related-organisms/scrub-typhus
- https://www.uptodate.com/contents/scrub-typhus-treatment-and-prevention
- Gavin C. K. W. Koh, Richard J. Maude, Daniel H. Paris, Paul N. Newton and Stuart D. Blacksell. Diagnosis of Scrub Typhus. Am J Trop Med Hyg. 2010 Mar; 82(3): 368–370.
- Jennifer McQuiston. CDC. Rickettsial (Spotted & Typhus Fevers) & Related Infections (Anaplasmosis & Ehrlichiosis). Chapter 3. Infectious Diseases Related to Travel.
- David H. Walker. Scrub Typhus — Scientific Neglect, Ever-Widening Impact. N Engl J Med 2016; 375:913-915. DOI: 10.1056/NEJMp1608499.
- Thomas Weitzel, Sabine Dittrich, Javier López, Weerawat Phuklia, Constanza Martinez-Valdebenito et al. Endemic Scrub Typhus in South America. N Engl J Med 2016; 375:954-961. DOI: 10.1056/NEJMoa1603657
- The Centre for Health Protection, Department of Health. Typhus and Other Rickettsial Diseases.
- Philippe Parola, Pr Philippe Brouqui and George Watt. Orientia tsutsugamushi (Scrub Typhus). Antimicrobe.
- Yuehong Wei, Yong Huang, Lei Luo, Xincai Xiao, Lan Liu and Zhicong Yang. Rapid Increase of Scrub Typhus: An Epidemiology and Spatial-Temporal Cluster Analysis in Guangzhou City, Southern China, 2006–2012. PLoS ONE 9(7): e101976. doi:10.1371/journal.pone.0101976.
- Sirisanthana V, Puthanakit T and Sirisanthana T. Epidemiologic, clinical and laboratory features of scrub typhus in thirty Thai children. Pediatr Infect Dis J. 2003 Apr;22(4):341-5.
- http://www.vdh.virginia.gov/epidemiology/epidemiology-fact-sheets/scrub-typhus-fever-mite-borne/
Similar Posts:
- Histoplasma Capsulatum – Habitat, Morphology, Epidemiology, Virulence Factors, Treatment + More
- Cryptococcus Neoformans – Habitat, Morphology, Epidemiology, Virulence Factors, Treatment + More
- Hepatitis B Virus- Structure, Epidemiology, Symptoms, Pathogenesis, Diagnosis, Treatment and Vaccines
- Techniques of Virus Cultivation
Can we perform culture and susceptibility testing of this parasite,to rule out resistance pattern of antimicrobial drugs? Please suggest.